
Medically reviewed by Dr. Heba Al Tarhuni, D.D.S., Olive Tree Dental, London, Ontario
Go and look at your kid right now, while they’re on the couch or reading or watching something. Not talking. Just resting.
Are their lips together?
If the answer is no, and if the answer has been no for a while, that’s worth ten minutes of your attention. Not panic. Attention.
Most parents never think to look
And why would you? Nobody tells you to check. Your child breathes, they’re growing, they seem fine.
But the mouth is a backup system for breathing. The nose is the primary one. When a child breathes through their mouth most of the day and all night, they’re running on the backup, and the body starts adapting around it. Those adaptations are the part I care about as a dentist, because a lot of them show up in the jaw, the bite, and the teeth.
I see the results in my chair constantly. Crowded teeth. An open bite that orthodontics alone won’t hold. A child who’s tired at 9am. By the time it reaches me, the mouth breathing has usually been going on for years, and no one connected it to anything.
What actually goes wrong?
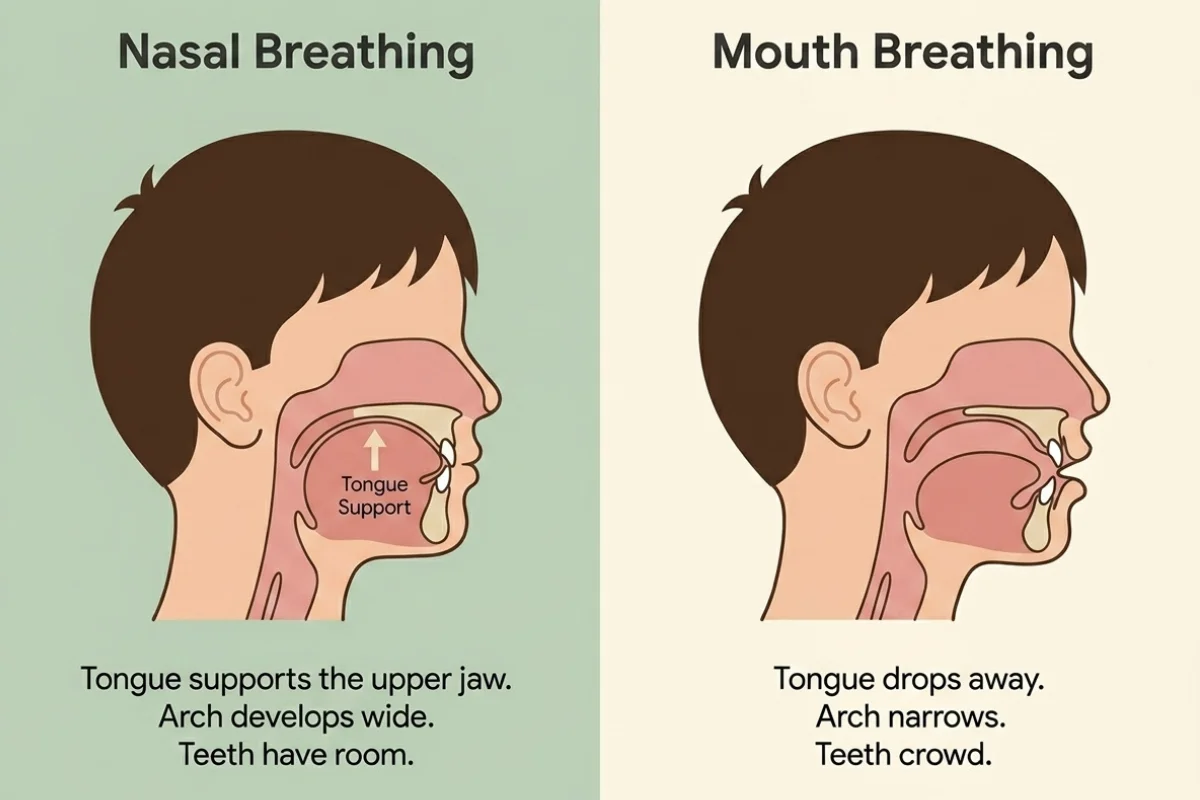
When the tongue sits in the roof of the mouth, which is where it belongs at rest, it acts like natural scaffolding. It gently shapes the upper jaw outward as the child grows. That wide, well-formed arch is what gives adult teeth room to come in straight.
Now take that scaffolding away. To breathe through the mouth, the tongue has to drop down and forward, out of the palate. It stays there. All day. All night. For years.
The upper jaw grows narrower than it should. Adult teeth arrive with nowhere to go, so they crowd and overlap. The tongue, sitting low and pushing forward, presses against the front teeth every time your child swallows. We call that a tongue thrust, and over hundreds of swallows a day it can hold the front teeth apart so they never fully bite together.
That’s an open bite. And here’s the frustrating part: you can straighten those teeth with braces, but if the tongue is still pushing forward every swallow, the teeth tend to drift back toward where they were. The muscle pattern outlasts the orthodontics.
The signs, and where parents get it wrong
Here’s what to watch for:
- Lips apart at rest. The single most reliable sign, and the easiest to check.
- Snoring. Children should not snore. It is not cute and it is not normal.
- Restless sleep. Sheets destroyed by morning. Odd sleeping positions with the head tipped back.
- A dry mouth or bad breath first thing. Air moving over the gums all night dries out the saliva that normally protects the teeth.
- Waking up tired despite a full night in bed.
- Daytime crankiness, trouble focusing, or difficulty settling.
- Chapped lips that never quite recover.
- Grinding teeth at night.
- Dark circles under the eyes in a child who genuinely gets enough sleep.
Now, the thing parents get wrong.
When a child breathes through their mouth all night, their sleep gets fragmented. They don’t sleep deeply. And an exhausted child does not act like an exhausted adult, who gets quiet and slow. An exhausted child gets wired. Distractible. Emotionally short-fused. Bouncing off the walls at bedtime.
So it looks like a behaviour problem. It gets treated like a behaviour problem. And nobody checks the breathing.
I’m not saying every restless child is a mouth breather. I’m saying it’s on the list, it’s checkable, and it’s very often missed.
The face thing, since you're going to search it anyway
If you’ve been reading about this, you’ve probably run into the phrase “mouth breathing face,” usually somewhere alarming.
Let me be measured about it, because this is exactly where the internet goes off the rails.
There is a real, well-documented relationship between long-term mouth breathing during the growth years and how the jaw and face develop. A narrower upper jaw, a longer lower face, lips that don’t close comfortably, a chin that sits back. It is real, and it is one of the reasons we take this seriously in children rather than waiting.
What I won’t tell you is that your child’s face is ruined, or that this is irreversible, or that any single product fixes it. That’s fear, not dentistry, and there’s a lot of it online right now.
What I will tell you is that jaws grow for a long time, that growing bone responds to how it’s used, and that the earlier you address the cause, the more of that growth you have to work with. That’s the honest version. It’s also the more useful one.

Adults, before you scroll past
Everything above applies to you too, just on a longer timeline.
If you snore, wake with a dry mouth, feel unrefreshed after eight hours, or had braces as a teenager and watched your teeth slowly drift back, the muscle pattern is worth investigating. Adults don’t have growth on their side the way children do, but the tongue and facial muscles can absolutely be retrained. And adults tend to be far more consistent with the exercises than eleven year olds are, which counts for a great deal.
What we actually do about it
The first job is finding the cause, because “stop breathing through your mouth” is useless advice if the child physically cannot breathe through their nose.
Sometimes the airway is genuinely blocked. Enlarged tonsils or adenoids. Chronic allergies. A structural issue in the nose. If that’s what’s going on, no exercise programme in the world will fix it, and the right move is a referral to an ENT or your family doctor. We’d rather send you to the right person than sell you the wrong treatment.
Sometimes the nose is perfectly clear and the mouth breathing has simply become a habit. The airway got blocked once, years ago, the child adapted, the blockage resolved, and the pattern stayed. Muscles are stubborn like that.
And sometimes it’s a restriction under the tongue, a tongue tie, that never let the tongue reach the palate in the first place.
Once we know which of those we’re dealing with, the treatment follows. Where the muscle pattern is the problem, that’s where myofunctional therapy comes in. It’s a structured programme of exercises that retrains the tongue, lips and facial muscles: getting the tongue back up to the palate at rest, restoring nasal breathing, and correcting the swallow.
It sounds almost too simple. It works because it’s targeting the actual cause instead of the symptom. It is not quick, it depends heavily on doing the exercises at home, and consistency matters more than intensity. Anyone promising a fast fix is overselling.
For infants and young children where a tongue tie is restricting movement, a release may need to come first, so that the tongue can actually get where the exercises are asking it to go.
What it costs, and the insurance thing nobody explains
We don’t publish prices, and I want to be straight about why. Two children with identical-looking symptoms can need completely different treatment: one needs an ENT referral and nothing from us, another needs a tongue tie release plus a full therapy programme. Quoting a number before assessing would be guessing, and I’m not going to guess with your money.
For general Ontario context: an initial orofacial myofunctional assessment commonly runs somewhere in the range of $150 to $250 across the market, and a full multi-session therapy programme typically falls between roughly $1,400 and $2,400 depending on length and complexity. Those are broad market ranges, not our fees, and they’re here so you’re not walking in blind.
Now the part that actually saves people money.
Most insurers do not recognise “myofunctional therapy” as a category at all. Look for it on your benefits statement and you will not find it. What they respond to is the diagnosis, not the label on the treatment. Coverage frequently runs through speech therapy benefits rather than dental ones, because the underlying issue involves swallowing and oral function.
So when you call your provider, don’t ask “do you cover myofunctional therapy?” You’ll get a no. Ask whether your plan covers therapy for swallowing, speech or breathing disorders, and ask what documentation they need. That single change of wording is the difference between a denial and a claim, and almost nobody tells parents this.
We’ll give you the documentation. Ask us for it.
The part I'd like you to take away
You don’t need to diagnose anything. That’s my job.
You just need to look at your child when they’re not thinking about it, and notice whether their lips are together. If they aren’t, and if you’re also seeing the snoring, the wrecked sheets, the morning tiredness, the crowded teeth, then it’s worth a conversation.
Jaws grow. Habits set. The window is wide open and then it isn’t. Nothing here is an emergency, but it is one of those things where earlier is meaningfully easier than later.
We’re at 759 Richmond Street, in downtown London, at the corner of Oxford and Richmond. If you’ve read this far because something rang true, book an assessment and bring your questions. Or call us on (519) 672-0931 and ask.
Bring the observations too. You’ve been watching this child sleep for years. You know more than you think you do.
Frequently Asked Questions
It can be both, and that’s exactly why it’s worth checking. Long-term mouth breathing during the growth years is associated with changes in how the upper jaw develops, which can affect crowding, bite and sleep quality. Sometimes it’s driven by a blocked airway, and sometimes the blockage cleared long ago and the habit stayed. Those need different treatments, so the assessment matters.
Bring it up as soon as you notice it. Because so much of this is tied to jaw growth, there’s a real advantage to addressing it while the child is still growing. That said, we assess and treat adults regularly too, so it is never pointless to ask.
Research supports myofunctional therapy as one useful part of managing sleep-disordered breathing, including mild to moderate obstructive sleep apnea, by improving the tone and position of the tongue and airway muscles. It is not a standalone cure and it does not replace a sleep study or a diagnosis from a physician. It works best alongside proper medical assessment.
Usually not under that name. Insurers typically don’t list myofunctional therapy as a benefit category. Coverage more often comes through speech therapy benefits, because the therapy addresses swallowing and oral function. Phone your provider and ask specifically whether your plan covers therapy for swallowing, speech or breathing disorders, and ask what documentation they need. We can help provide it.
Very much so, and this is one of the more important questions here. If a tongue thrust or mouth breathing pattern is left in place, the muscles can gradually push the teeth back out of alignment after the braces come off. Addressing the muscle pattern is often what protects the orthodontic result long term.
Programmes commonly run over several months, with regular sessions plus short daily exercises at home. The home practice is the part that determines the outcome. It is a slow, steady retraining process rather than a quick fix, and consistency matters far more than intensity.
Author byline
Medically reviewed by Dr. Heba Al Tarhuni, D.D.S. Dr. Heba earned her Doctor of Dental Surgery at the Schulich School of Medicine & Dentistry, graduating on the Dean’s Honour List. She completed a Pediatric Mini-Residency in Toronto and has pursued advanced training in pediatric dentistry and orthodontics. She is a Senior Master Provider in FASTBRACES® and is certified in clear aligner therapy including Invisalign and ClearCorrect. Born and raised in London, Ontario, she treats children and adults at Olive Tree Dental, 759 Richmond Street.
Olive Tree Dental has been voted a Top Choice Dental Clinic in London, Ontario for five consecutive years (2022 to 2026) and holds a 4.9 star rating across 500+ Google reviews.